Feature Contents:Feature Article
Feature article: Toward an exit strategy [1] – Booster vaccinations –
The following article provides a summary of the results of analysis conducted after the resolution of the fifth wave of infections, focusing on exit strategies for the pandemic with a view towards medium- to long-term containment of infection. In particular, the following presents the views at the time on measures regarding vaccinations.
Introduction
At present, the fifth wave has been brought under control in Japan and the infection situation is relatively stable. On the other hand, it is still necessary to consider measures that allow economic activity to recover and prevent infections spreading again in the medium to long term.
There are thought to have been multiple factors involved in bringing the fifth wave under control, including the thorough implementation of basic infection protection such as vaccinations, avoidance of risk behaviors, masks and avoidance of the “Three Cs,” as well as seasonal factors. At the same time, a fundamental difference with the previous phase of spread and control has been the rapid progress of vaccinations, which suppressed infections to a level far lower than during the previous phase of control. Although the start of vaccinations was slower than other countries, as a result of continuing vaccinations at more than one million a day for about three months from June, as of October 20, the rate of vaccinations administered to the total population has reached more than 76% for the first dose and more than 68% for the second dose. 1.
Meanwhile, there is continued debate on how far the rate of vaccination of the total population should be raised to prevent infections from spreading again, and when booster doses should be given in view of the reduction in vaccine efficacy over time.
On this AI simulation project, multiple researchers have been using various methods and models to analyze scenarios with similar assumptions in order to consider the situation from multiple perspectives. The analytical results obtained on issues like those above are shown below.
※It should be noted that the following are the results of calculations and simulations by researchers, and not the official opinion of the national government.
1 Rate of vaccination to prevent infections from spreading again
- Infections spreading extensively again will occur only with difficulty if Japan continues behavioral restrictions with a rate of vaccination of 80% or more of the total population
- Greater abolition of restrictions would require a rate of vaccination of at least 85% of the total population (if children aged 12 years or younger are not vaccinated, a rate of vaccination should be in excess of 90% of the population aged 12 years or older)
The declaration of a state of emergency has been lifted and although not yet back to their pre-COVID level, flows of people are becoming more active and it is conceivable this.
tendency will strengthen at the end of the year. In addition, it has been pointed out that the effects of the vaccines wane over time 2. Three levels of preventive effect are expected from the vaccines: infection prevention; sickness prevention; and aggravation prevention. IgG antibodies in blood are involved in infection prevention and sickness prevention, and it is thought that a reduction in those antibodies is linked to the waning of these effects. Immunological memory due to B cells and T cells plays an important role in aggravation prevention, not just IgG antibodies, so even if blood IgG antibodies decrease, aggravation is prevented by the action of killer T cells, which eliminate cells infected with the virus at the same time as B cells produce antibodies promptly after infection. Because of this, even if the infection prevention effect decreases along with IgG antibodies after vaccination, the fact that the decline in aggravation prevention is limited compared to the infection prevention effect is due to this kind of immunological mechanism. Simulations are being carried out focusing also on infection prevention effects at the same time as aggravation prevention effects. This is because reducing the risks of people who have not been vaccinated and people still at high risk even if they have been vaccinated due to immunodeficiency or an underlying disease is important. That is because it is conceivable that a means will be required to suppress the overall state of infections when the waning of vaccination effects is expected (the waning of sickness prevention and aggravation prevention in particular). Roughly what rate of vaccination is required to prevent infections spreading again in the future in anticipation of this kind of change in situation?
Figure 1 is an analysis assuming that people’s comings and goings will be activated (increase in opportunities for contact) to about the same level as last year. Simulations were carried out with final vaccination rates against the total population of 70%, 75%, 80% and 85% in consideration of the waning over time of vaccine antibody effects.
It is suggested from this analysis that infections equivalent to a fifth wave could occur if restrictions on activities were abolished at a vaccination rate of 80%. The results show that a vaccination rate of at least 85% is required for the complete abolition of restrictions on activities.
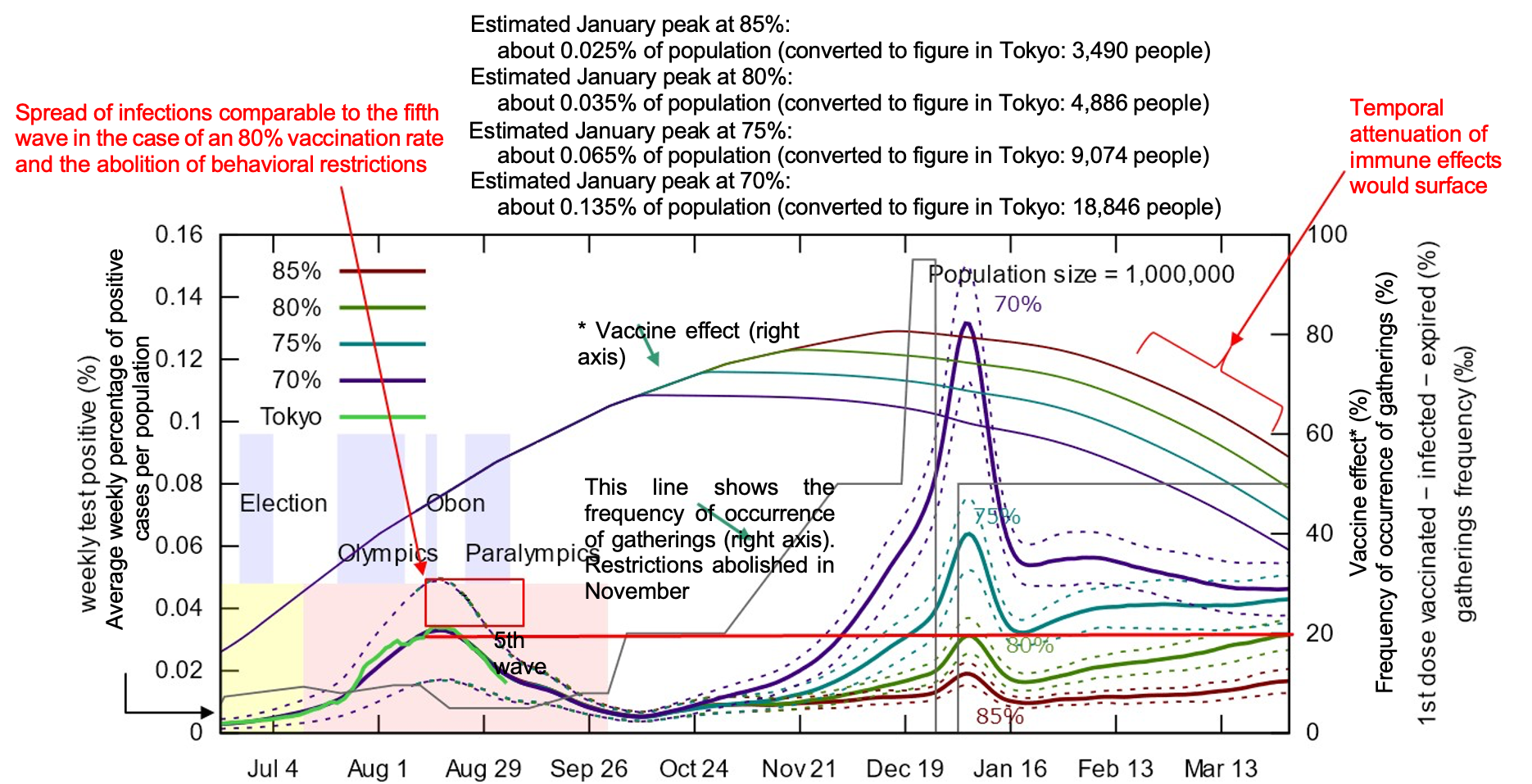
Figure 1: Simulation of the number of new infections in Tokyo if behavioral restrictions were abolished (rate of vaccination: 70%, 75%, 80%, 85%) (analysis by Professor Unemi, Soka University) 3
Related Research: RQ4,: “Lifting of the 4th declaration of a state of emergency and subsequent scenarios,”(https://www.covid19-ai.jp/ja-jp/presentation/2021_rq3_countermeasures_simulation/articles/article140/)
Requiring a rate of vaccination of 85% or higher is expected to have the same effect in suppressing the number of severely ill cases and similar results have been obtained under other models covered in this AI and simulation project (link).
2. For example, the latest research includes the following papers. Gold berg, Y. et al., Waning Immunity after the BNT162b2 Vaccine in Israel, New England Journal of Medicine, October 27, 2021 DOI: 10.1056/NEJMoa2114228
3. It was assumed here that the protective effect of the vaccine against infection disappears 214 days after the second vaccination, but it should be kept in mind that it is not actually clear at present whether the effect decreases to the level of “disappearance.” However, the time scale of this simulation runs approximately to the level of halving and does not include the region where the effect disappears. As discussed in Chapter 3, caution is required over the fact that there have been multiple different reports on the attenuation of infection prevention effects.
2 Rate of vaccination seen from the medium to long-term trend in the number of infections
- If the final rate of vaccination is 75% or 80%, Japan may repeat large waves of changes over the next five years.
- A rate of vaccination of 85% or higher is required to prevent infections spreading again in the medium to long term
Looking at the increase in the flows of people towards the end of the year, a rate of vaccination of 85% of the total population is required to prevent infections spreading again. In addition, in order to consider the future recovery of daily life over the medium to long-term, it is necessary to consider strategies anticipating the situation in several years’ time, not just the state of infections after three months.
Figure 2 shows analysis of the final rate of vaccination, vaccination protection effect and basic reproduction number after setting baseline (black), optimistic (blue) and pessimistic (red) patterns. (The details of the parameter values are shown below the figure and for further details, please refer to the linked individual report.)
The results of this analysis suggest that a vaccination rate of 75% or 80% will see infections fluctuate greatly and repeatedly over five years, whereas a vaccination rate of 85% will suppress the number of new infections over the long-term.
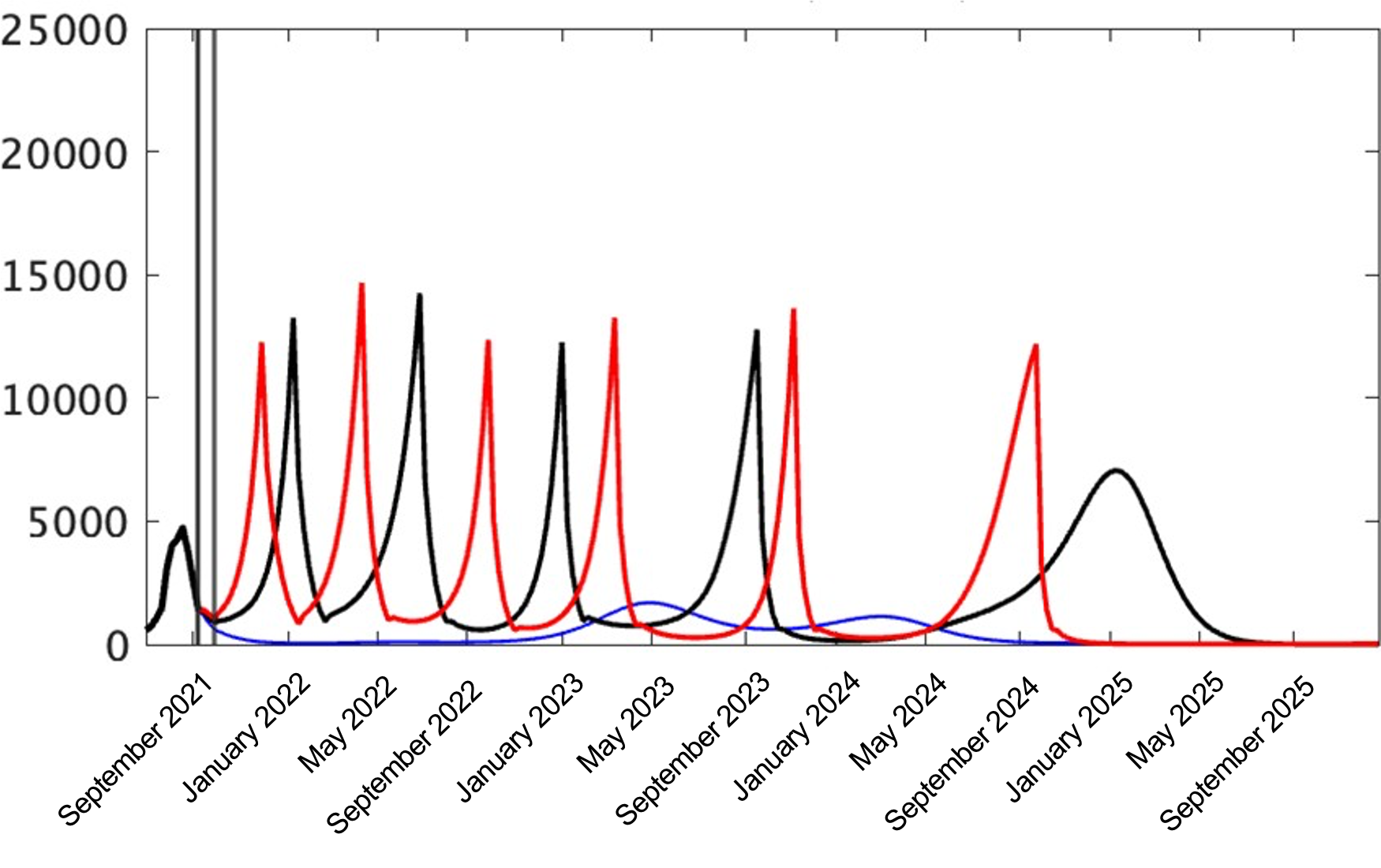
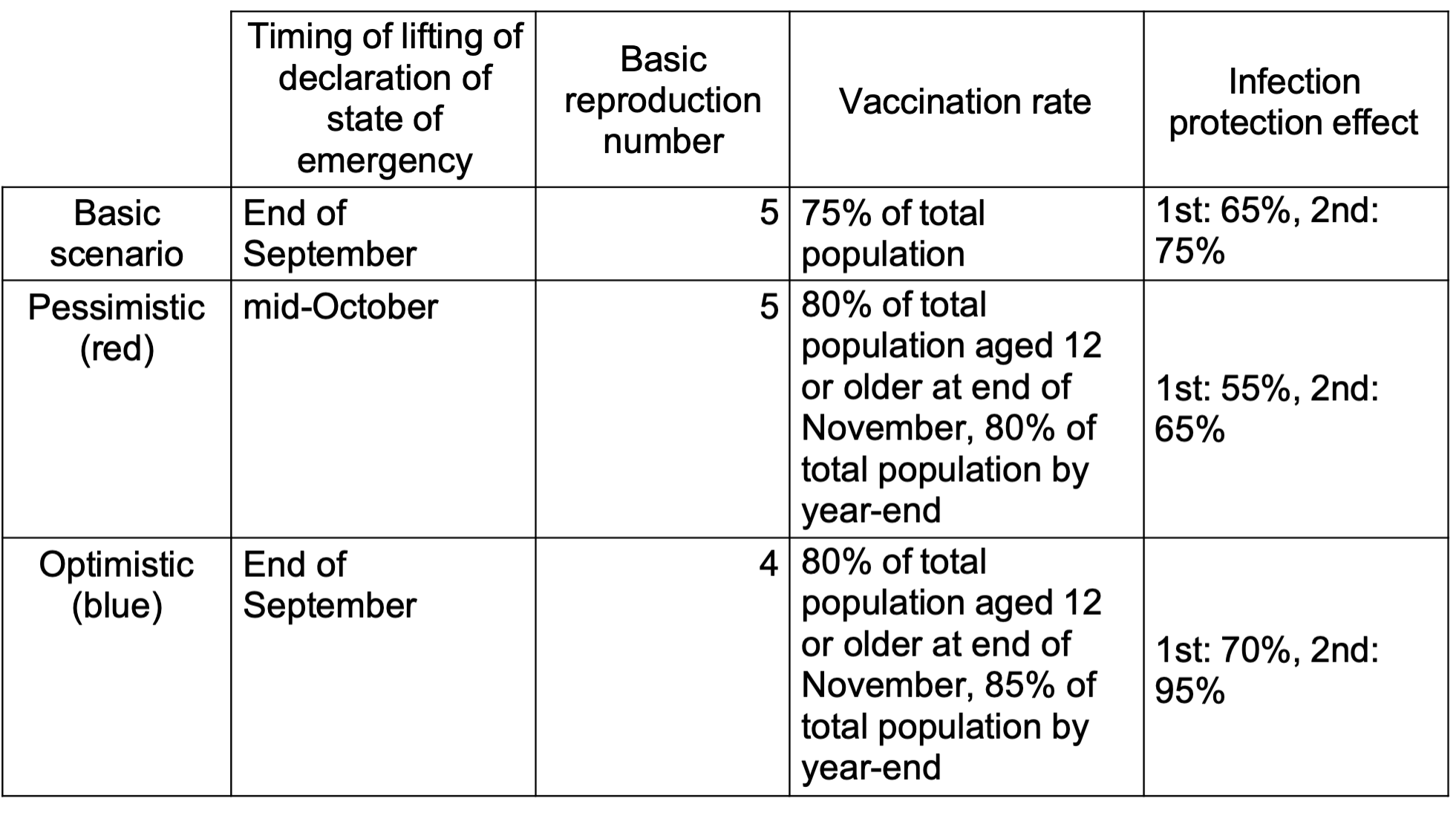
Figure 2: Number of new infections in Tokyo over the next five years: base scenario (black), optimistic (blue), pessimistic (red) (analysis by Associate Professor Nakata, the University of Tokyo)
Related research: RQ4: “The world after completion of vaccination: COVID-19 infections and long-term economic prospects #2,”(https://www.covid19-ai.jp/ja-jp/presentation/2021_rq3_countermeasures_simulation/articles/article147/)
In fact, even though Singapore has a vaccination rate of more than 80%, it is assumed that 80% is insufficient because the numbers of infections and critically ill people have increased rapidly under the relaxation of behavioral restrictions. In the case of Singapore, because infections were suppressed to a very low level, there are very few people with immunity due to infection so it can be assumed that the people with immunity are basically those who have been vaccinated.
In addition, in Europe, which was hit by a major spread of infections, Portugal reached a vaccination rate of 85% of its total population recently and figures are currently trending steadily with 1,000 positive cases and a few deaths each day among a population of 10 million people. However, if these figures are converted to the Japanese population, the level would be 10,000 positive cases and several dozen deaths each day. Spain has reached a vaccination rate of 80% and is maintaining a level of about 3,000 positive cases and 20 to 30 deaths each day. In Europe and elsewhere, it is necessary to include in calculations not only vaccines, but also the large number of people who have acquired immunity through infection.
In addition, the reality is that even if the vaccination rate is 85%, it will not be 85% uniformly and infections will spread in areas and groups where there are many unvaccinated people.
From our simulation results and the cases of these countries, it is thought that a final vaccination rate of at least 85% of the total population is required in order to maintain the numbers of infections and severely ill persons at a certain level after a significant lifting of behavioral restrictions. The basic reproduction number for the delta strain, currently the dominant COVID-19 strain, was reported to be equivalent to chickenpox, but it seems reasonable to estimate that it is equivalent to rubella or, tentatively, about five . In Japan, the prevalence of antibodies to rubella, which is supposed to have a basic reproduction number of 5 to 7, is about 95% in women aged 18 years and older, but about 80% in men, and as a result, epidemics are recurring . Considered from these perspectives, it is understood that achieving and maintaining extremely high antibody prevalence is required to form herd immunity.
Apart from vaccines, there are antibody cocktails and oral drugs that are expected to be approved in the future that will assist in preventing increased severity of disease, but these have not been considered in the present simulation because of their limited supply. The preventive effect of vaccines against increased severity of disease is supposed to be about 90%, that of antibody cocktails is 70%, and among oral medicines, that of Merck’s molnupiravir is about 50% and that of Pfizer’s Paxlovid is about 90%. It will be necessary to incorporate conditions assuming the supply and prescription systems for antibody cocktails and oral medicines are established as future model parameters. In particular, the approval and supply systems from this winter to next spring are not clear, and it cannot be described as appropriate to incorporate these regimens into simulations for the time being.
However, in Japan, where a vaccination rate of about 80% of the total population can be expected, it will be essential to devise ways to vaccinate several percent more, and at the same time, to construct a medical treatment pipeline that also includes these therapeutic and preventive drugs. A simulation based on a comprehensive prevention and treatment pipeline as a simulation for this construction is a future issue.
4. CDC warns that delta variant is as contagious as chickenpox and may make people sicker than original Covid
(https://www.cnbc.com/2021/07/30/delta-cdc-warns-variant-is-as-contagious-as-chickenpox-may-make-people-sicker.html)
6. Ying Liu, Joacim Rocklöv, The reproductive number of the Delta variant of SARS-CoV-2 is far higher compared to the ancestral SARS-CoV-2 virus, Journal of Travel Medicine, Volume 28, Issue 7, October 2021, taab124,https://doi.org/10.1093/jtm/taab124
7. Infectious Disease Surveillance Center, National Institute of Infectious Diseases, “The present state of rubella and future rubella countermeasures”http://idsc.nih.go.jp/disease/rubella/rubella.html
8. MERCK AND RIDGEBACK’S INVESTIGATIONAL ORAL ANTIVIRAL MOLNUPIRAVIR REDUCED THE RISK OF HOSPITALIZATION OR DEATH BY APPROXIMATELY 50 PERCENT COMPARED TO PLACEBO FOR PATIENTS WITH MILD OR MODERATE COVID-19 IN POSITIVE INTERIM ANALYSIS OF PHASE 3 STUDY>=
(https://www.merck.com/news/merck-and-ridgebacks-investigational-oral-antiviral-molnupiravir-reduced-the-risk-of-hospitalization-or-death-by-approximately-50-percent-compared-to-placebo-for-patients-with-mild-or-moderat/)
9. PFIZER’S NOVEL COVID-19 ORAL ANTIVIRAL TREATMENT CANDIDATE REDUCED RISK OF HOSPITALIZATION OR DEATH BY 89% IN INTERIM ANALYSIS OF PHASE 2/3 EPIC-HR STUDY
(https://www.pfizer.com/news/press-release/press-release-detail/pfizers-novel-covid-19-oral-antiviral-treatment-candidate)
3 Timing of booster vaccinations in accordance with antibody attenuation
- Simulation suggests that even with the introduction of vaccine-test packages, infections will spread depending on the timing of booster vaccinations.
- Results of analysis concerning booster vaccinations show that it is most effective for the doctor to ascertain the timing after judging that immunity obtained from the second dose has weakened and infection has become possible
Increasing the rate of vaccination to at least 85% of the total population is necessary to prevent infections spreading again most recently and in the medium to long term, but in order to maintain this effect, it is necessary to also consider booster vaccinations based on the decrease in vaccine effects over time.
This point has also been considered in combination with complementary measures based on vaccine-test packages, the timing of implementation of which is currently being discussed. These are measures assuming that there is a certain level of people who retain antibodies due to vaccines so it is important to ascertain the timing of booster vaccination measures against the attenuation of antibodies over time.
In an Israeli study, increased risks of infection and severity of illness were observed five months after vaccination (Figure 3). Based on these results, it is preferable for booster vaccinations to be given around five months after the second vaccination, and if possible, the doctor should judge the timing of the booster vaccination by measuring the IgG antibody titer of each individual.
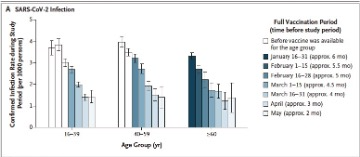
Figure 3: Data on attenuation of effects after vaccination in Israel (Goldberg, et al, Waning Immunity after the BNT162b2 Vaccine in Israel, New England Journal of Medicine, October 27, 2021)
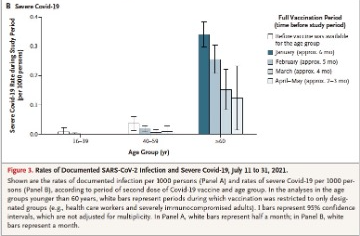
Figure 4 shows a simulation of the case in which booster vaccinations are given to all generations after 180 days. The upper part of Figure 4 shows the case where booster vaccinations are not given and the lower part shows the case where they are given from 180 days. Both the number of positive cases and the number of severe cases are greatly reduced, but the reduction in the number of severe cases is particularly striking.
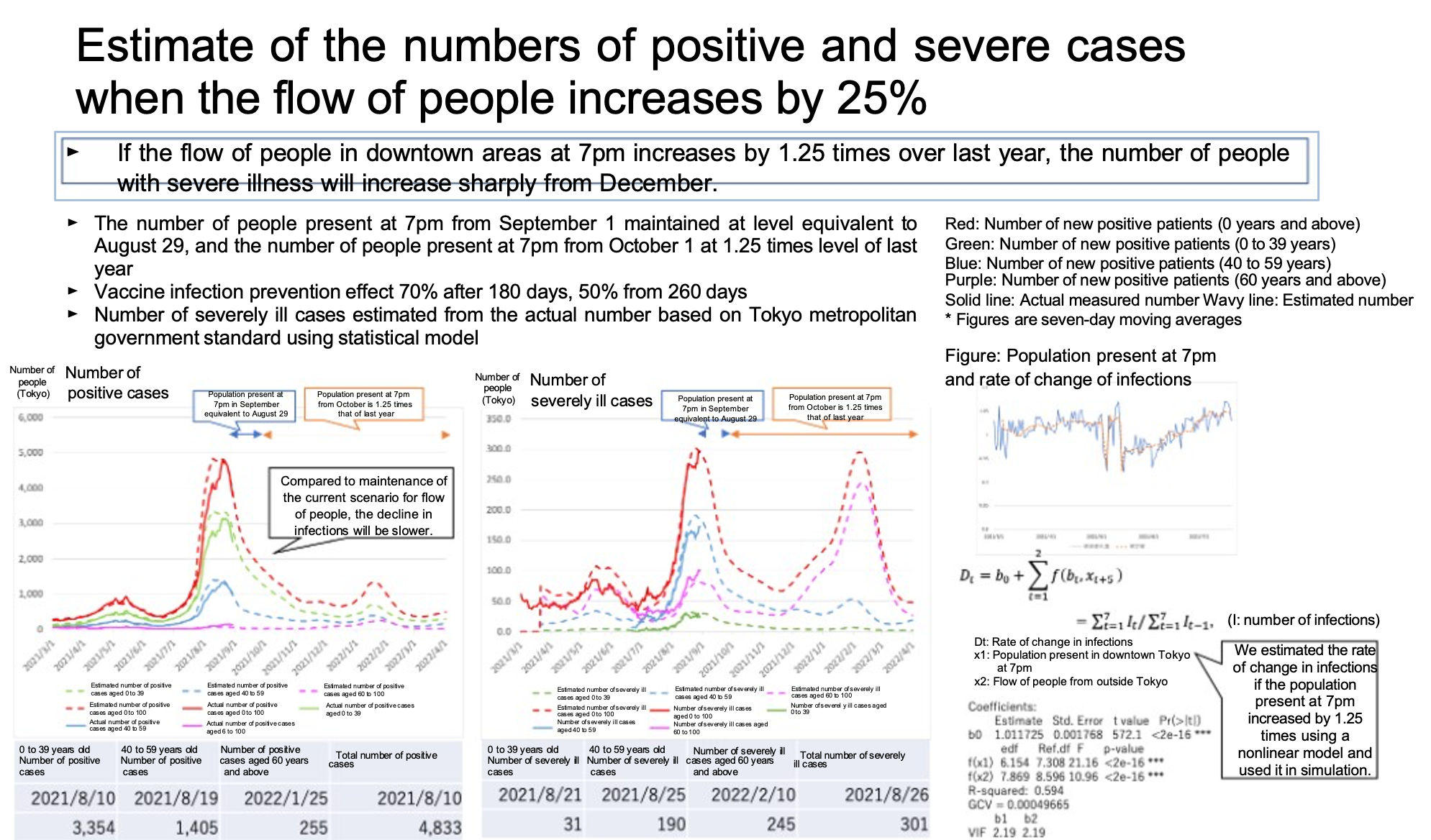
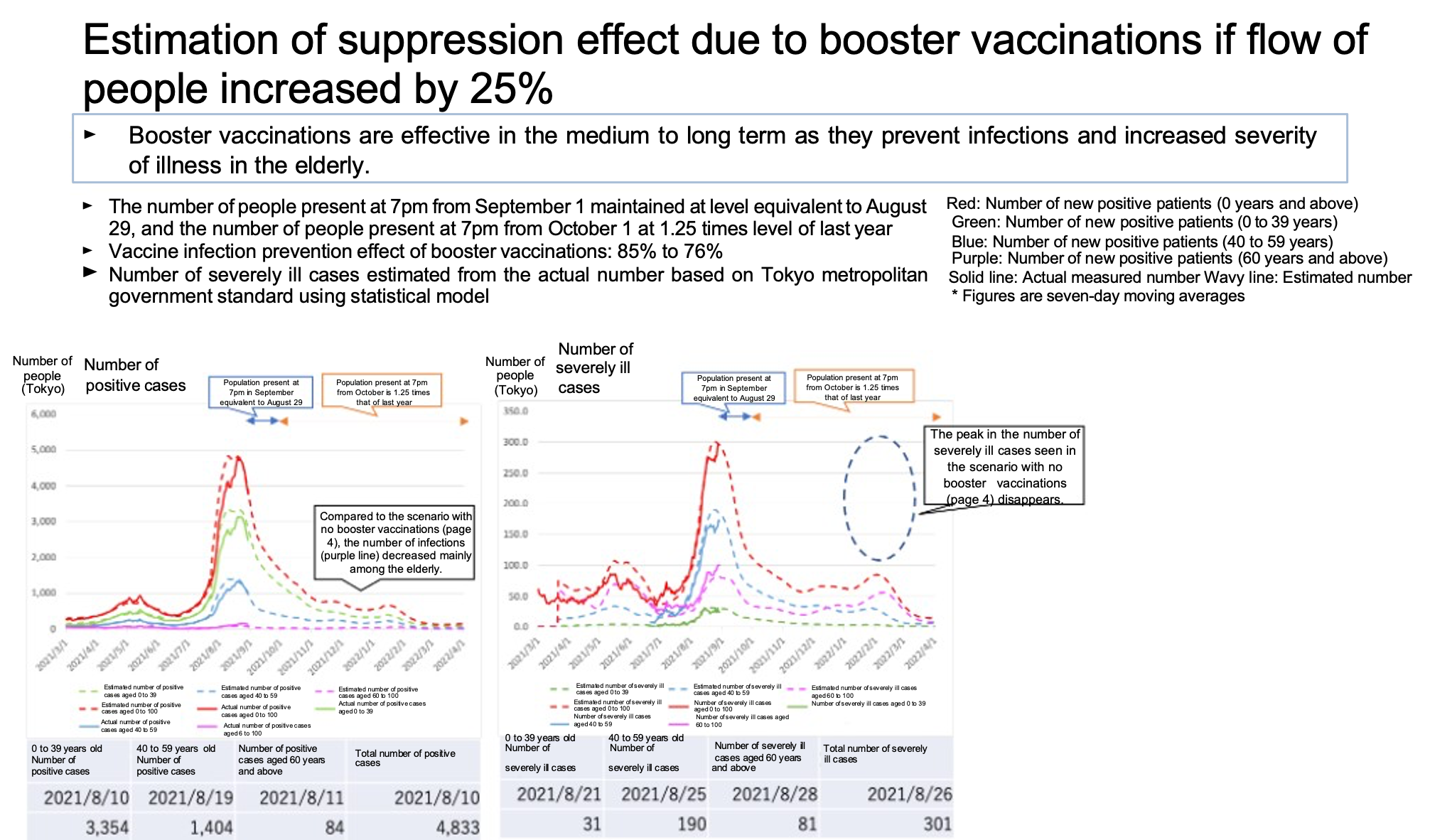
Figure 4: Effect of booster vaccinations when flows of people increase
(analysis by Professor Kurahashi, University of Tsukuba)
https://www.covid19-ai.jp/ja-jp/presentation/2021_rq3_countermeasures_simulation/articles/article142/
Figure 5 shows the results of analysis of trends in the number of new infections in Tokyo based on the timing of booster vaccinations under the condition of a vaccine-test package being introduced. The results of this analysis suggest that infections could spread again if booster vaccinations are given six or eight months after the second dose, even in a situation where confirmation of vaccination history (vaccine passport) shows interpersonal contact among non-holders decreases by 50%. This is because with uniformly given booster vaccinations in the case where it is assumed the state of immunity after vaccination differs for each person, the risk of infection in people whose immunity has weakened early will increase. On the other hand, the results of analysis show that the spread of infections is suppressed when booster vaccinations are given after the doctor has judged antibody attenuation.
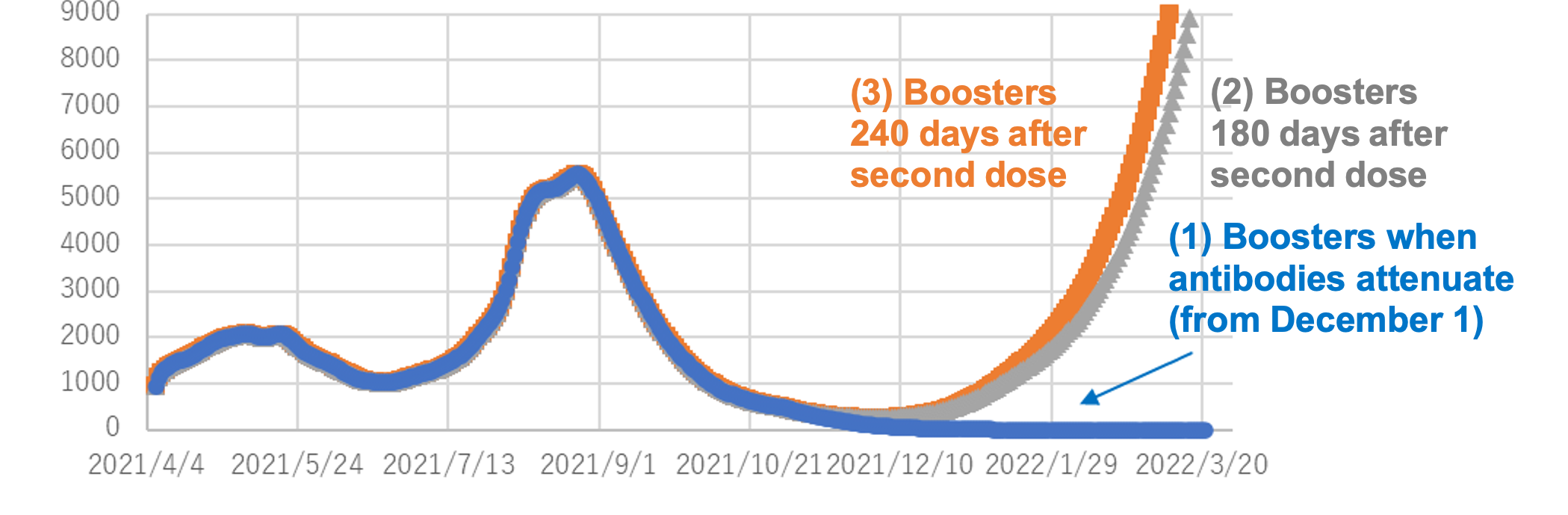
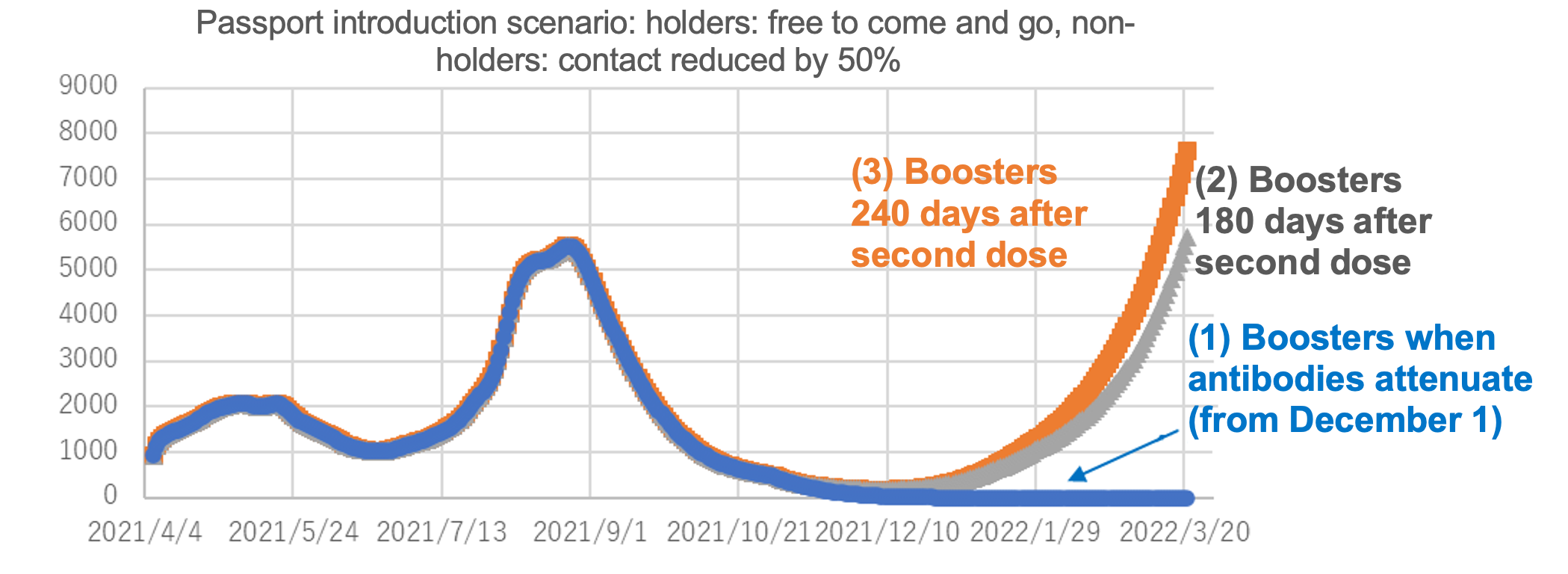
Figure 5: Number ob new infections in Tokyo by confirmation of vaccination history(vaccine figure) introduction scenario
(analysis by Professor Osawa, the university of Tokyo)
https://www.covid19-ai.jp/ja-jp/presentation/2021_rq3_countermeasures_simulation/articles/article143/
It has also become known that there are large individual differences in immune status after vaccination. At the same time, there have also been multiple reports on the weakening of immunity. Apart from the abovementioned Israeli study, a US study11 suggests that the infection protection effect due to vaccines weakened to 50% by four months after the second dose. In a Canadian study, although the effect weakened, a 90% infection prevention effect was maintained to five months, but decreased to 75% after 6 months12. However, what is consistent is the result that the vaccine effect weakens greatly about six months after the second dose.
On the other hand, studies have also been presented showing that stronger immunity can be induced by a longer interval between the first and second vaccination doses, and if this also applies to the interval between the second and third doses, people with a certain level of immunity induced could choose a longer dosing interval13.
This time, we have presented findings obtained from the results of analysis to this point on vaccination rates and booster vaccinations, which will be essential to exit strategies. On the other hand, there are also difficult aspects to increasing vaccination rates for various reasons such as age restrictions. In addition, our simulations also suggest that even after booster vaccinations, vaccine-test packages and basic infection prevention measures need to continue for the foreseeable future. Therefore, multiple measures are required, not just vaccinations, including vaccination record and test packages, and the establishment of supply and prescription systems for preventive and therapeutic drugs.
ワクチン接種記録・検査パッケージについては「出口戦略へ②」で記載する。
10 Gold berg, Y. et al., Waning Immunity after the BNT162b2 Vaccine in Israel, New England Journal of Medicine, October 27, 2021 DOI: 10.1056/NEJMoa2114228
11 Tartof, S., et al., Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: a retrospective cohort study, Lancet, 398: 1407-16, 2021 (この報告の研究期間中にデルタ株の割合が増えていることはデータを見る上での留意事項である)
12 Skowronski, D., et al., Two-dose SRAS-CoV-2 vaccine effectiveness with mixed schedules and extended dosing intervals: test-negative design studies from British Columbia and Quebec, Canada, medRxiv 2021(https://www.medrxiv.org/content/10.1101/2021.10.26.21265397v1.full.pdf)
13 Payne, R. et al., Sustained T Cell Immunity, Protection and Boosting Using Extended Dosing Intervals of BNT162b2 mRNA Vaccine, Cell, 184: 5699, 2022.
※The simulation introduced in this article is aimed at considering the effects of measures that can be taken under scenarios that can be assumed at the time using various models, and is not aimed at estimating the number of infected people, etc.
1 https://www.kantei.go.jp/jp/headline/kansensho/vaccine.html